
Always Consult Your Equine Veterinarian
Prevalence of Gastric Ulcers







Key Points
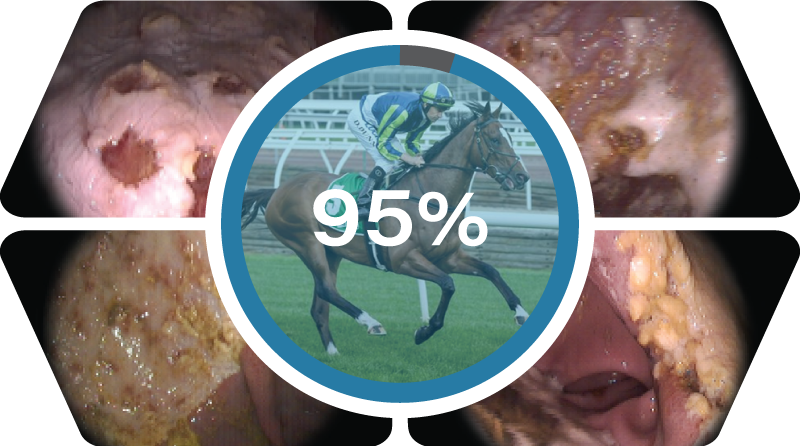
Gastric ulcers occur < 95% of thoroughbred and standardbred racehorses in training.

- Gastroscopy is the only definitive way to diagnose gastric ulcers and to monitor the effectiveness of any treatment or prevention programs.
- Horses should always be fed a high roughage feed of at least 2L/1.5kg prior to exercise to prevent "acid splash". Less than 10% of ulcers heal spontaneously.
- The horse's stomach has two parts. The top Squamous (white) part and a bottom glandular (pink) part. Both parts may develop ulcers but the treatment and prognosis for the two types are different.
- Omeprazole is the drug of choice for treatment and prevention of gastric ulcers in the racehorse1,2.
- Omeprazole should always be given on a relatively empty stomach and a minimum of 30 min (preferably 60 min) prior to feeding.
- Ensure horses do not chew on enteric-coated ulcer medications (eg Gastropell Forte & Gastropell Daily). Chewing may partially destroy their protective coating.
- Nutraceuticals, herbal extracts and compounded products for the treatment of gastric ulcers seldom meet their label claims1.
- Ulcers may recur once treatment has stopped. Most horses require ongoing treatment with ulcer medications such as omeprazole, especially when they remain in training1.
- Glandular/pyloric ulcers affect about 40% of racehorses.
- Glandular/pyloric ulcers require long-term treatment with a combination of medicines, including omeprazole. Consult your vet. Without alterations in management or initiation of preventative therapy, ulcers may quickly return if horses remain in training1.
- Maintenance doses of anti-ulcer medications are unlikely to be sufficient to prevent recurrence of ulcers in horses in full training3.
- Wherever possible, horses should be given free access to hay or pasture for 16 hours per day.
- Hand feeding horses a small amount of lucerne hay immediately after they have cooled out after a race will reduce gastric acid damage and help restore energy and protein levels, aiding post-race recovery.
Impact on Performance
Although horses with gastric ulcers may still perform well, and for example win races, they will in general perform better once their ulcers are treated.
Gastric ulcers have the potential to impact significantly on performance. This has been confirmed in several scientific studies.
There is also a huge amount of anecdotal and clinical evidence 4,5 to support the negative effect of ulcers on performance. Horses with ulcers may still win races or perform, but they are likely to improve once their ulcers have resolved.
Gastric ulcers are known to result in:
- Earlier fatigue
- Lower oxygen uptake
- Shorter stride length
This is in addition to the well-recognised symptoms of:
- poor appetite
- weight loss / poor body condition
- behavioural changes (eg. nervousness, reluctance to work, jacking up, irritability, etc.)
- dull coat ("ulcer coat")
- mild, intermittent colic, esp. associated with eating
- windsucking/crib-biting
- diarrhoea
- chronic ulcers may even cause anaemia
All of the above will also impact performance
Management Strategies
- The harder the horse works and the longer the horse is in work, the more likely it is to develop ulcers and the more severe the ulcers are likely to be6.
- Horses that work more than four times a week are known to have a higher prevalence of glandular/pyloric ulcers.
- Decreasing the number of times per week that the horse works is a useful strategy in reducing the prevalence and severity of ulcers.
- Horses that have some physical contact with each other (in addition to visual contact) are less likely to develop ulcers6. Horses are more likely to develop ulcers if a radio is playing in the stable6.
- Turn out/pasture time will reduce the prevalence of ulcers1,3,6.
- The more roughage (hay/grass) in the horse's diet, the less likely the horse is to develop ulcers1,3,6.
- Ideally, horses should have access to hay for 16-24 hours1,3,6. Horses are designed to be continuous grazers. Most overseas racing stables in countries such as the USA, UK and Europe provide continuous, unlimited access to hay (usually meadow or grass hay).
- Lucerne hay is high in protein and calcium, both of which provide extra gastric acid neutralising (buffering) effects1,3. Lucerne hay is the hay of choice to aid in the treatment and prevention of gastric ulcers.
- It is essential that your horse is fed prior to exercise. About 2kg of roughage would be ideal. This includes walking exercise. Feed in the stomach not only absorbs any free gastric fluid ("sponge effect") but also forms a physical barrier to acid splash.
There is a correlation between the amount of grain that is fed and the presence and severity of stomach ulcers1,2,3,6.
- Grain is partially broken down to volatile fatty acids in the stomach and this adds to the acid burden. Obviously, manipulation of grain ratios in racing stables is difficult.
- Consideration should be given to utilising fats/oils as an alternative energy source to replace some of the grain in the horse's diet.
- Up to one cup (200mL) of oil can be given twice a day in the feed. The oil should be introduced slowly into the diet over a period of about 3 weeks, starting with 50mL twice daily.
- Corn oil has been shown to provide additional protection against gastric ulcers. However, any vegetable oil high in Omega-3 fatty acids is likely to be of benefit.
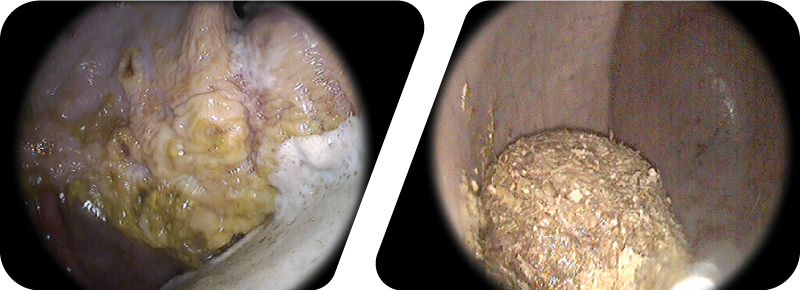
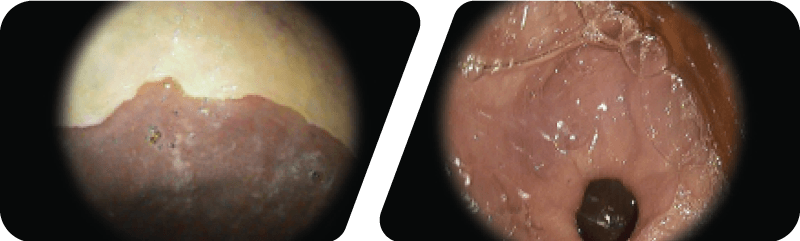
The image on the left / above shows a pool of gastric acid in a horse’s stomach. The stomach also has evidence of acid damage with yellowing of the lining and some deeper ulcers along the margo plicatus.
The image on the right shows the effect of feeding a roughage/hay feed. The food forms a “fibre sponge” ball which absorbs the gastric acid and also provides a physical barrier to acid splash.
Feeding a small roughage feed prior to working will minimise any gastric acid “splashing”.
Treatment Strategies
Ulcer medications must be given (30 to) 60 minutes prior to feeding, regardless of which ulcer medication is used.
- The presence of food in the stomach dramatically decreases the absorption of the ulcer medications (to as little as 15%).
- Ideally ulcer medications should be given at whatever part of the day the stomach will be mostly empty. It does not matter whether the medications are given in the morning or the afternoon.
- The time of administration should be tailored to fit into your daily stable routine. Prior to going on the walker in the afternoon or whilst the horse is being tacked up prior to work in the morning are good alternatives to first thing in the morning.
- Ulcer medications should be given at the same time every day, seven days per week.
Ulcer medications need to be given daily and long-term1.
- Horses that are in high intensity training/stressful scenarios (eg typical racing stable life) are at high risk of developing gastric ulceration and require regular and ongoing treatment for their ulcers.
- It is likely that ulcers may recur once treatment has stopped.
- In racehorses in full work, the full treatment dose is likely to be required. It is doubtful that the maintenance/prevention dose will prevent ulcers from recurring in this population of horses. Humans with gastric ulcers require ongoing (often life-long) treatment.
Omeprazole and ranitidine (both acid suppressing-drugs) are the only proven treatment for gastric ulcers in horses.
There is a large volume of scientific research and clinical experience proving that omeprazole is the most safe and effective treatment for gastric ulcers in horses.
- Omeprazole (eg Ulcershield, Gastropell) is 10 times more potent than ranitidine (Ulcerguard) and has been shown to be more effective than ranitidine in treating ulcers in horses6.
- Omeprazole comes in two forms; enteric-coated (eg Gastropell Daily and Gastropell Forte) and buffered paste (eg Ulcershield). Both formulations are known to protect the omeprazole against acid destruction in the stomach.
- Omeprazole only needs to be given once daily compared with ranitidine which is administered 2-3 times per day (ideally every 8 hours).
- Nutraceuticals, feed supplements and ulcer medicines seldom meet their label claims for the treatment or prevention of gastric ulceration2.
Glandular and pyloric ulcers
- Glandular/pyloric ulcers involve the bottom 2/3 of the stomach (the pink part) and the valve where the food leaves the stomach and enters the small intestine (pylorus).
- Symptoms caused by glandular/pyloric ulcers are similar to those of squamous ulcers.
- Glandular/pyloric ulcers are not caused by "acid splash" but acid suppression remains an essential part of their treatment.
- The treatment of glandular/pyloric ulcers is more problematical. They are difficult to clear up and require longer-term treatment (8-12 weeks). Your veterinarian can advise you of the best treatment options if your horse is diagnosed with pyloric ulcers.
Management of gastric ulcers in a racing stable should incorporate periodic gastroscopies.
- This will aid not only in the management of individual affected horses but also in general stable management.
- Gastroscopy is the only definitive way to diagnose and grade gastric ulcers.
- Pre- and post- gastroscopies are the only way to monitor the effectiveness of any treatment regimen.
Impact on High Performance
The $2.6M inch. The finish of the 2008 Melbourne Cup won by Viewed. Racing is a sport where an inch can mean the difference of thousands of dollars in prize money, not to mention prestige. Gastric ulcers are known to result in a lower maximum oxygen uptake, decreased stride length and a shorter time to fatigue, all of which adversely affect performance. Viewed was on anti-ulcer medications.
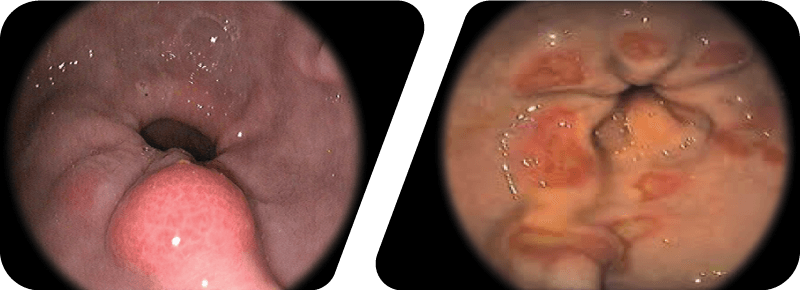
Up to 40% of racehorses will have ulcers/lessions of their pylorus (the valve that regulates the flow of ingesta from the stomach into the small intestine). Pyloric lessions may be inflammatory (left) or ulcerated (right).
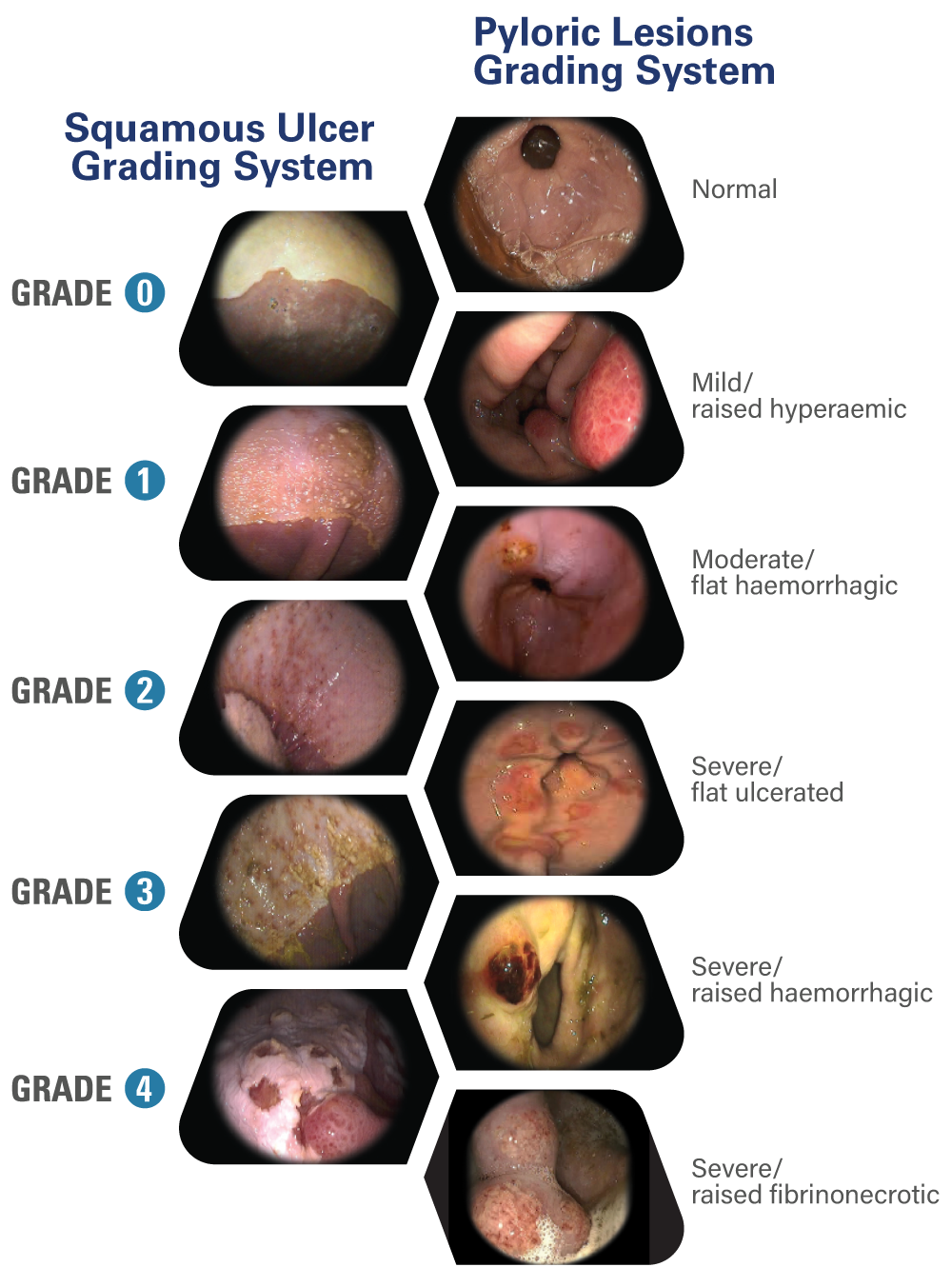
Grading Ulcers & Lesions
References:
1) Sykes BW, Hewetson M, Hepburn RJ, Luthersson N, Tamzali Y. European College of Equine Internal Medicine Consensus Statement - Equine Gastric Ulcer Syndrome in Adult Horses. J Vet Intern Med (2015); 29:1288-1299.
2) Zavoshti FR, Andrews FM. Therapeutics for Equine Gastric Ulcer Syndrome. Vet Clin Equine 33 (2017) 142-162.
3) Andrews FM, Larson C, Harris P. Nutritional
Management of gastric ulceration. Equine Vet Educ (2017) 29 (1) 44-55.
4) Nieto JE, Snyder JR, Vatisas NJ, Jones JH. Effect of gastric ulceration of physiologic responses to exercise in horses. Am J Vet Res (2009); 70:787-795.
5) Franklin SH, Brazil TJ, Allen KJ. Poor performance associated with equine gastric ulceration syndrome in four Thoroughbred racehorses. Equine Vet Educ (2008); 20:119-124.
6) Lester GD, Robertson I, Sercombe C. Risk factor for gastric ulceration in thoroughbred racehorses. Rural Industries and Development Corporation 2008 Australian Government publication 08/061.
©Content & edited by:
Dr. Michael Robinson
Global Technical Veterinarian, BVSc, PhD
Randlab
